
Why I Don’t Touch Copay Foundations
Maybe Because AFPs Take Up That Headspace? Maybe Because The IRA Cap Makes Them Feel Optional?

My client portfolio is divided into two buckets.
First, pre-launch biotechs who have just submitted their NDA or BLA, and need Patient Support strategy built from scratch.
Second, mid-cap teams who built something a few years ago and now want someone to take a look. Half the time, their program is fine. They just need leadership alignment.
The other half?
If they are running their own nurse team, there is always an opportunity.
Always.
Scratch that. It’s usually a failure to document and train on clear rules of engagement, document HCP or Patient engagements, and integrate those activities into the data infrastructure. Y’know… the usual.
I’m a solid advisor, but a lousy salesperson. 😉
Seven times out of ten, the program doesn’t need a rebuild. It needs a reset. Stronger intake criteria. Clearer roles. A less reactive operating model.
But I digress. Let’s get back to the folks looking toward a launch.
It’s not surprising that when we start planning for access, someone eventually brings up third-party Patient Assistance Foundations.
“Should we donate to a foundation?”
“Can we set one up?”
“Can you help us think through it?”
And my answer is always the same:
Nope. I don’t do that work.
Talk to Legal. Talk to Finance. Really.
This post is not advice.
It is not a strategy guide.
It is just a high-level overview.
(It is really not, but I am going to say it is.)
A Quick Word on What I’m Not Talking About
Let’s be clear.
When I talk about third-party foundations, I’m not talking about a Manufacturer’s Patient Assistance Program (PAP). PAPs are typically free goods programs for uninsured or underinsured Patients who meet specific income and eligibility criteria.
Different infrastructure.
Different compliance exposure.
Different operating model.
I help clients with PAPs all the time. (BTW, I also wrote a primer on PAPs here.)
I’m also not talking about commercial copay assistance, where the Manufacturer covers some or all of a Patient’s out-of-pocket cost for a drug after their commercial insurance coverage has been applied towards the purchase (or “claim”) of that medicine.
Enrollment for commercial copay support usually happens in one of three ways:
Via a brochure or card handed to the Patient in their doctor’s office or included in the starter kit
Digitally, when the Patient visits the brand’s website and answers basic yes/no questions about insurance type and product use
Through a hub portal or pharmacy microsite, where a support team or pharmacist enrolls the Patient electronically behind the scenes
Assistance is typically limited to commercial Patients for on-label use of a medication, as prescribed by a U.S.-based healthcare provider (HCP). Most programs require Patients to attest that they’re not on a government-funded plan. (I’ll get into “why no government Patients” a bit further down.) Some even block participation at the pharmacy level based on BIN/PCN codes or eligibility logic built into the portal.
These programs aren’t new. They’re standard in access planning.
What I’m talking about here is something very different:
Manufacturer donations to third-party foundations: often serving Medicare Patients, often for high-cost therapies, and always under regulatory scrutiny.
How These Foundations Work (Plain and Simple)
Third-party charitable foundations are 501(c)(3) nonprofits that provide financial assistance to Patients struggling with medication and healthcare costs. Many of them:
Operate disease-specific funds
Offer copay, insurance premium, or travel support
Primarily serve Patients who are insured, often through Medicare
May have separate pathways or programs for uninsured Patients, depending on the fund
Open and close based on the availability of donations
These programs are designed to help Patients.
They are not designed to serve Manufacturer pull-through or access metrics.
And it gets trickier in rare diseases.
If you’re the only Manufacturer with an approved treatment for a condition, and a foundation just so happens to open a fund for that condition? That’s not neutral. That’s not even subtle. Even with the best of intentions, your donation can look like an access workaround.
The compliance exposure is real. So is the reputational risk.
Many of these foundations operate on a large scale, representing multiple therapeutic areas. The dollar amounts are staggering. We’re talking, collectively, billions of dollars per year. With a “B”. Some process hundreds of thousands of grants and calls each year. Some issue prepaid debit cards. Some pay premiums directly to insurers. All of them live in compliance-first environments with matching infrastructure. (Well, if they’re not, they should be, or they’ll be *very* sorry.)
If you want to support their mission, great.
Just do not confuse “support” with “leverage.”
Even with the zillions and zillions (note: I’m taking creative liberty using a “z” instead of a “b”), these Foundations can and do (often) run dry.
Don’t believe me?
Try calling into a foundation serving rheumatology Patients in early February.
The Coverage Gap That Foundations Fill
Commercially insured Patients often have access to Manufacturer-funded copay support programs.
Government-insured Patients do not.
If a Patient is on Medicare, Medicaid, TRICARE, or any other government-funded plan, they are ineligible for commercial copay assistance. That exclusion exists to protect the government’s best price under Medicaid law and federal anti-kickback statutes.
Which is one reason these foundations exist. They are often the only safety net for Patients on public insurance who are still expected to cover thousands in out-of-pocket costs.
So, when a Manufacturer tries to shut down the idea of foundation support entirely? They are ignoring a structural gap that commercial assistance simply cannot fill.
But Wait, What About the IRA? MP3? OOP Smoothing?
Starting in 2025, Medicare Part D out-of-pocket costs are capped at $2,000 per year.
On paper, that is a game-changer.
In practice, it is already prompting some Manufacturers to rethink their donation strategies altogether.
If Medicare Patients will never owe more than $2,000, do you still fund the foundation?
Do you shift support toward behaviorally sticky moments, such as first-fill abandonment or mid-year discontinuation?
Do you still need multiple layers of eligibility criteria?
Some are staying the course. Others are pivoting. But everyone’s asking the same question:
“What’s our role once the ceiling drops?”
This isn’t just a Patient win.
It is a planning reset.
And it’s one that’s already making Finance, Legal, and Access leads revisit the role of foundation donations.
And One More Operational Headache
Nothing will make a Market Access lead more frustrated than discovering that their hub vendor (or an internal support team) is bypassing the Manufacturer’s own commercial copay program and sending Patients to a foundation instead.
Before you go, “Huh? That’s not right.”
Lemme tell you: I’ve seen this happen with my own eyes.
Medical benefit product, successful line extension, warehoused demand, and the commercial copay vendor’s operations went off the rails. The case managers at the Hub began to see Foundations as a workaround.
Ay yay yay.
It happens all the time.
Why? Because it’s fast. Or easy. Or a fund happened to be open that day.
But now your commercially insured Patient is off your branded card, out of your tracking system, and back into the wild.
Worse? You might still be paying for hub services, claims processing, or field team time for a Patient who’s no longer on your program.
It is not always malicious. But it is often sloppy.
And it undercuts your access strategy more than anyone wants to admit.
Meanwhile, most Manufacturers only point Patients to the foundation's contact information on the brand.com/patient webpage.
Warm transfer a Patient to a Foundation? Big compliance no-no.
Call into the foundations daily to check if the funds are open or closed?
I don’t know a Hub that doesn’t do this.
Why I Stay in My Lane
I am not against charitable foundations. I think they are essential.
But when it comes to Manufacturer donations, the regulatory landscape is specific, evolving, and risky if you are not working with the right experts.
This is why I stay in my lane.
I do not help Manufacturers thread the compliance needle.
I do not give advice about donation timing, structure, or fund targeting.
I do not help anyone disguise a forecast as philanthropy.
You need Legal Counsel who lives and breathes this space.
You need Finance to model what happens if a program backfires.
If your team does not already have this alignment, that’s your first step.
Not a donation.
There is history here. And it is not subtle.
The Department of Justice has investigated it. (Multiple. Times. Keep reading.)
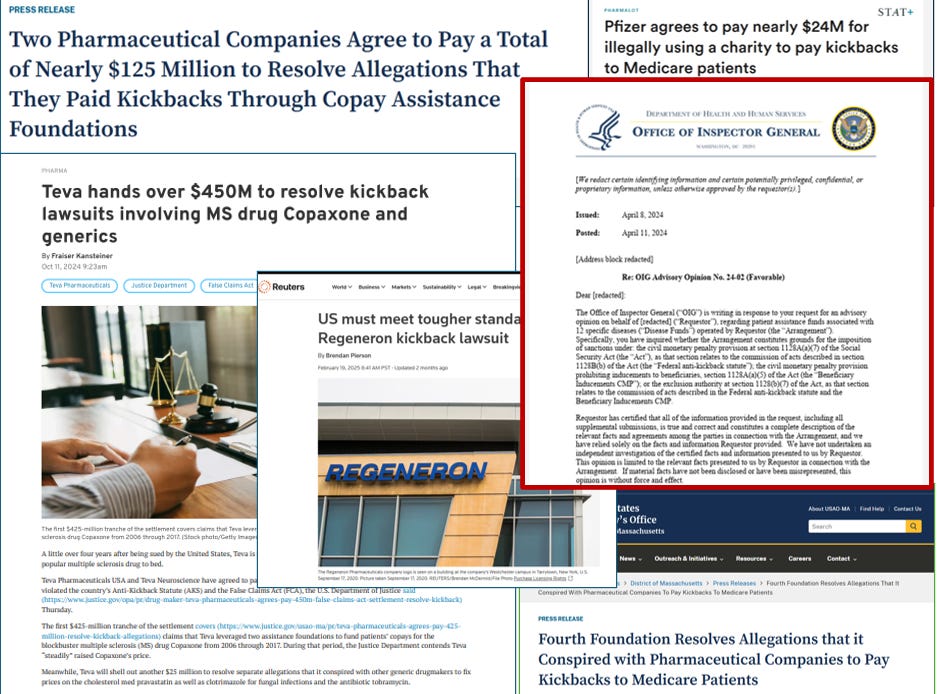
The Office of Inspector General has issued guidance.
Multiple Manufacturers have paid settlements.
If you are going to play in this space, get the right people in the room.
The View From the Patient Side
It is easy to get lost in compliance language and funding logistics and forget why these programs matter in the first place.
Ask any Patient or Caregiver what it feels like when a fund opens… then closes within hours.
Ask what it feels like to refresh a foundation’s website every day, hoping a fund reopens before a prescription runs out.
Ask about the panic when a specialty pharmacy says, “We can’t ship until you get new authorization.”
Ask what happens when a grant runs out and the out-of-pocket cost is still unaffordable.
This is not theoretical. It happens every single week in oncology, neurology, rheumatology, rare diseases, and beyond.
And if your access strategy depends on a foundation being funded, open, and available at the exact moment a Patient needs help?
You are not planning. You are gambling.
What the Data Say
According to the 2025 State of Patient Access Report, published by one of the largest independent foundations:
23 percent of Patients say that their prescription medicines are not affordable
More than 40 percent of Patients with cost issues delayed care, skipped doses, or went into credit card debt
More than one out of 3 Patients worry about being able to afford their medicines in the future
These are not fringe cases. These are Patients trying to survive chronic and life-threatening illnesses with cost-sharing structures that were never built for reality.
Another Reason I Stay Out of This Lane
If the historical record was not enough, recent litigation should make it crystal clear.
In early 2023, a major Manufacturer tried to establish a Medicare copay assistance program for a cardiovascular drug. The Supreme Court declined to hear the case, leaving in place a ruling that said the arrangement would violate federal anti-kickback laws.
That same company then won a related class action brought by private insurers. The case alleged that the Manufacturer's past donations to foundations induced use of branded drugs over lower-cost alternatives. The court dismissed the case. But that was not the end of the story.
Back in 2018, that same Manufacturer paid $23.8 million to settle with the government over allegations it used a foundation to cover Medicare copays for three of its own drugs in violation of the False Claims Act.
And then there is Teva.
In 2024, Teva paid $450 million to resolve claims that it used two charitable foundations to cover copays for Medicare Patients of its multiple sclerosis drug, Copaxone. While Patients were shielded from rising costs, Teva raised the price and allegedly coordinated donations to match projected need.
The government called it inducement. Teva called it independence. The case ended in one of the largest settlements of its kind.
Still think this is a gray area?
The risk is not theoretical.
The line is not blurry.
And there are better ways to support Patients than ending up in a headline.